|
Iliotibial band syndrome (ITBS) has been reported as the second most common running injury and most common reason for lateral (outer) knee pain in runners. In case you were wondering, a large research study reported patellofemoral pain syndrome to be the most common running-related injury. What is your ITB? The iliotibial band is a thick band of fascia that runs on the outer side of the thigh. It is a dynamic and multidimensional structure with relationships that span the lumbar spine (lower back) to the anterolateral (front and outer) aspect of the knee. The ITB connects through the gluteus maximus to the lumbar fascial tissue; and down to the femur (thigh bone), the outer quadriceps muscle (vastus lateralis), the outer hamstring muscle (biceps femoris), and anterolateral tibia (shin bone). The interactions of the ITB suggest an interactive relationship between these different structures. 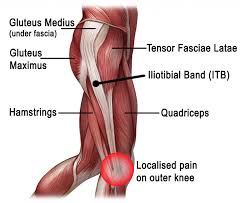 Diagnosis and Typical Symptoms The diagnosis of ITBS is based on clinical examination – patients typically present with tenderness over the lateral femoral epicondyle and report a sharp, burning pain when the practitioner presses on the lateral epicondyle during knee flexion and extension. The pain is particularly acute when the knee is at 30° of flexion. The onset often occurs at the lateral knee after a few miles of running, or hiking long distances. Walking with the knee extended can relieve the symptoms, and downhill walking or running can aggravate symptoms. Theories and Causes There are two main theories behind ITBS: the compression model and the friction model. The ITB inserts in the region of the femoral epicondyle and it glides over the lateral femoral epicondyle when the knee bends. It is thought that due to biomechanical imbalances, the ITB can either become compressed or there is increased frictioning (rubbing) which causes pain and inflammation. Scientific literature often suggests there is there an overlap between these two models. There is no one single cause of ITBS in runners, however, research has shown that biomechanical factors such as increased hip adduction (movement towards your mid-line), knee internal rotation, and femur (thigh bone) external rotation can contribute. Muscle weakness in the hip abductor and/or external rotators can be involved, as well altered neuromuscular control, or poor running technique leading to pelvic drop or rotation. This highlights how ITBS is actually preceded by numerous biomechanical issues, and that the lateral knee pain itself is often the end symptom that you become aware of. On a positive note, these biomechanical issues have the potential to be corrected with physiotherapy, and this also emphasises the importance of sound biomechanics in the first place, which can help to prevent these types of running injuries. Your physiotherapist can help to reduce your injury risk by assessing your movement control and providing you with a plan to improve your biomechanics. Management One key biomechanical goal is to reduce strain related to excessive lengthening of the ITB and stress related to the insertion at the lateral femoral epicondyle. In the initial stages (up to 2-weeks), anti-inflammatory medication and ice is recommended, along with a reduction in your running volume and intensity, and avoid downhill running. Physiotherapy manual treatment for ITBS may include myofascial treatment addressing trigger points in the biceps femoris, vastus lateralis, gluteus maximus, and tensor fasciae latae muscles. In addition, acupuncture/dry needling techniques can prove helpful. Physiotherapy will also aim to address walking and running re-training, particularly looking to correct pelvic drop, pelvic rise, and trunk deviation if present. ITB stretches can be useful, but you may also need to stretch various muscle groups around the hip and pelvis, such as the quadriceps, gluteals or hamstrings (if appropriate). Core strengthening exercises (particularly gluteus medius exercises) and progressive resistance exercises will be given to improve biomechanics and motor control. Movement control tests such as the single leg squat, the step down test, and single leg dead lift can help to provide baseline measures from which to improve. If localised pain persists at the lateral femoral epicondyle, an ultrasound-guided corticosteroid injection could be considered. You can discuss this further with your physiotherapist. Return to Running When your exercises are pain-free and you can achieve them with good form, this is a good indication that running can be recommenced. A guideline for this is 6-weeks though the range is variable based on successful completion of the earlier phases of recovery. Graded progression is achieved by running every other day with emphasis on good running form, and initially may include easy sprints on level ground. Downhill running is not recommended in the first 2-weeks, and an emphasis on movement control is recommended to focus on pelvic control, forward trunk, and softer landing. Should you wish to discuss any aspects of this or book an appointment with one of our therapists please get in touch. References
Baker, R. L. and Fredericson, M. 2016. Iliotibial Band Syndrome in Runners: Biomechanical Implications and Exercise Interventions. Phys Med Rehabil Clin N Am 27(1), pp. 53-77. doi: https://doi.org/10.1016/j.pmr.2015.08.001 Fairclough, J. et al. 2006. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. Journal of Anatomy 208(3), pp. 309-316. doi: 10.1111/j.1469-7580.2006.00531.x Taunton, J. E. et al. 2002. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med 36(2), pp. 95-101. doi: 10.1136/bjsm.36.2.95
2 Comments
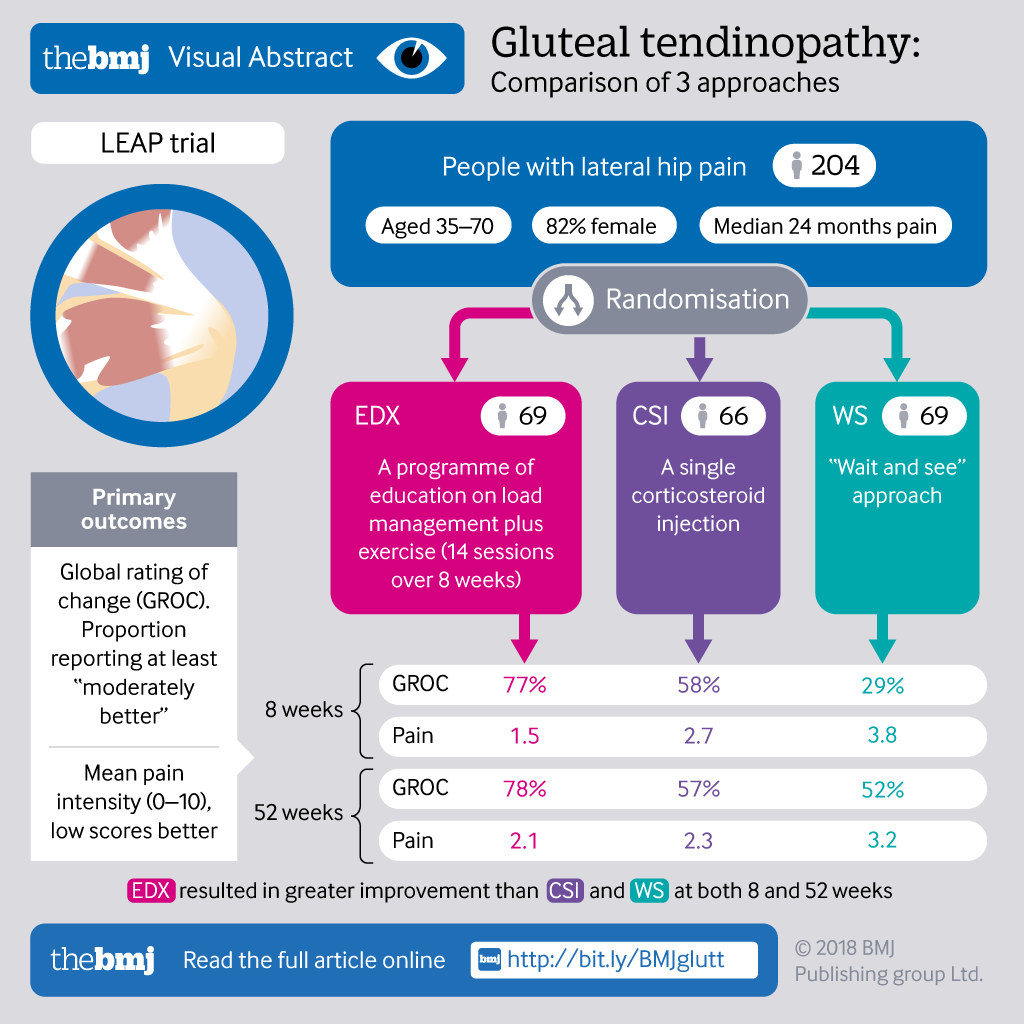
So what is a Gluteal Tedninopathy (GT)?
 How common is it:
Signs and Symptoms:
Top tips for managing GT pain:
Exercise therapy:
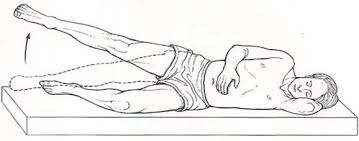 2. Lie on your side with your knees bent. Tighten your pelvic floor muscles and gently pull your lower stomach in. Lift your top knee as far as you can, without letting your pelvis rotate forward or back. Keep your feet together during the exercise. 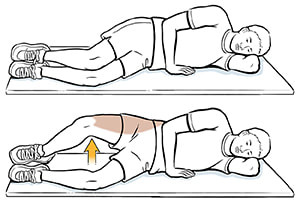 New evidence: Hot off the press!
 When assessing soft tissue injuries, whether that’s muscle, tendon, ligament or nerves, I’m looking for what brings on your symptoms. It can include basic everyday movements like bending forward to do your shoelaces, looking down at your phone or just sitting on the sofa. Usually during an examination, I’ll ask the patient to move into the position that causes the pain, which gives me a good idea of what type of injury has developed. The majority of soft tissue problems I see are caused by over-used muscles that result in the body producing tough, dense scar tissue that builds up. Eventually muscles become shorter, tendons become inflamed and nerves can become irritated. I have found that Active Release Technique (ART®) is a fantastic tool for the management of these conditions. ART® uses manual therapy to apply compressive, tensile and shear forces to address repetitive strain injuries, cumulative trauma injuries and constant pressure tension lesions. Its design is 3 fold:
 I treated a patient recently who had suffered shooting pain down their leg for the last 3 months. They
visited PhysioImpulse seeking assessment for a suspected disc bulge. After the initial assessment it turned out to be chronic irritation of a muscle around their hip which I treated with a combination of manipulation and ART®. This initial session alleviated the shooting leg pain and with a few more follow up sessions the localised hip pain had resolved fully restoring the patient back to normal pain free activities. If you have persistent pain feel free to give us a call and book in for your initial consultation to assess if ART® is the solution for you. Parkinson’s Disease is a progressive neurological condition, which can cause a number of symptoms that impact on walking, balance and everyday tasks. An area of the brain known as the substantia nigra normally produces dopamine, which is a chemical that transmits signals to another part of the brain responsible for coordinating movement. When a person has Parkinson’s, there is less dopamine produced, which can cause the following symptoms:
Neurological physiotherapy is extremely beneficial for patients with a diagnose of Parkinson’s Disease. Our experienced physiotherapists will create a treatment plan with you tailored towards your specific goals and needs. Treatment can be in clinic or as a home visit if required. Treatments can include:
Have a look at the latest Parkinson’s Disease blog on PD Warrior. PD Warrior PD Warrior is a relatively new and exciting treatment concept started in Australia and now used all over the world to improve the symptoms of Parkinson’s Disease. It is based on the latest evidence and research and consists of a programme of rehabilitation that is specific to a person’s Parkinson’s symptoms. It can be tailored to each person and works through key movement patterns and has been shown to slow down disease progression. Unlike other exercise-based treatments, PD Warrior works ensures that treatment is tailored to specific difficulties that a person may be experiencing that are directly related to the condition. By doing this, goals can be worked towards more effectively. PD Warrior can be used with any age group and can be tailored to the stage of Parkinson’s Disease that a person is at. Patient Experience Darren was diagnosed with idiopathic Parkinson’s Disease at age 65. He had been finding that his walking had slowed down considerably over the past 18 months and often tripped when going up stairs at home. After a number of tests and visits to specialists, he was seen by a neurologist who gave the diagnosis of Parkinson’s Disease. Darren loves to walk and would happily walk in the countryside for up to 10 miles. 2 months after his diagnosis, he decided to try neurological physiotherapy as he was desperate to get back to his local walking group. Darren had a combination of hands on treatment to address his stiff muscles and joints and also started the PD Warrior exercise programme, which he could also do at home in between physiotherapy sessions. He is now able to walk 5 miles including hills with his walking group and his neurologist has arranged his appointments once a year rather than the initial 6 monthly reviews. He has had no trips or falls in the past 6 months and feels more active and energetic than before his Parkinson’s diagnosis! Please contact Physioimpulse to book an assessment or contact Katie our specialist neurological physiotherapist for further details. Have a look at the video below describing PD Warrior. https://youtu.be/Hy02Ka-rsKs The benefits of running are countless, from weight management to disease prevention (Harris, 1981). Unfortunately these benefits can be offset by injury. Annually it is seen that up to 65% of people experience pain as a result of running (Marti et al, 1988). For this reason, it is essential to put in place preventative strategies to reduce the probability of injury. Common strategies include rest, painkillers, injections and even surgery. These approaches may improve the symptoms in the short term but are likely to fail tackling the root cause resulting in a re-injury (Noakes, 1991).
As summer approaches and better weather is arriving, there is nothing quite like going for a run. To ensure your running is as pleasurable and pain free as possible why not take advantage of the running analysis service we offer here at Physioimpulse. What is running analysis? Running analysis is the assessment of running technique. It highlights abnormalities within running gait with the result of preventing or at the very least limiting running injuries. What to expect We run 60 minute sessions, during which we will take video recording of your running technique. We record multiple angles to ensure we capture all possible abnormalities, these include videoing from the front, side, back and also specifically your feet. We then assess each of these videos with you in slow motion, highlighting potential issues which may in time result in injury or reduced running efficiency. Benefit of having your running analysed by Physioimpulse We also complete a physical assessment and combine thiswith the information gained in the running analysis to create a bespoke exercise program. This effective combination alongside tailored manual therapy allows us to better prevent injury and improve running performance. In addition to this we can make recommendations on different types of footwear which may benefit you. We can also refer you on to our specialist gait analysis and orthotics service, where customised inserts can be created for you. To find out more, read this Page What is PGP? PGP (previously known as Symphysis Pubis Dysfunction (SPD)) affects 20-50% of all pregnant women. PGP is localised around the back of the pelvis, and described as a pain between the posterior iliac crest (the back of the pelvis) and the gluteal fold (the line where the buttock meets the thigh), particularly around the sacroiliac joint (SIJ). The pain may radiate down the back of the thigh and can also occur in conjunction with/or separately of pain in the symphysis (a cartilaginous joint located between the left and right pubic bones near the front midline of the body, just in front of the bladder). PGP can cause pain and stiffness in the pelvic joints, difficulty walking, climbing stairs and turning in bed. Common painful areas:
Pelvic girdle pain has been explained as the result of a combination increased pelvic joint mobility, mechanical strain, and altered neuromuscular control, which also affects the myofascial structures around the sacroiliac joints and the symphysis pubis. Causes Several factors have been identified as potential risk factors for PGP, including a history of previous low back pain, trauma of the back or pelvis, the number of previous pregnancies, high levels of stress, emotional distress, physically demanding work, smoking and high body mass index (BMI). This does not mean that if you have one or more of these factors you will automatically develop PGP as every women and every pregnancy is unique. However, having an understanding of potentially contributing factors can help you to take more care of yourself. Management PGP can be treated by a physiotherapist because it is a mechanical joint problem rather than a hormonal problem. Manual therapy can consist of gentle mobilisations of the pelvis and spine and soft tissue release techniques such as massage and myofascial release. Mobility exercises, postural re-education and core stability/pilates exercises are very beneficial to get your muscles working properly so that they can support your lower back and pelvis. Other management techniques include the use of a pelvic belt, which helps to reduce pelvic pain and improve comfort of pregnant women by providing gentle compression and support. Some research has shown that the narrow flexible belts allow a decrease in SIJ and overall pain; and the broader and more rigid belt can help to decrease back pain but ultimately it is important that individuals choose the style of belt that is most comfortable and offers support where they feel they need it. Women can also talk to their GP or local pharmacist about pain relieving medications. From a physiotherapy point of view, pain relief can prove very helpful in the initial instances if individuals feel that they are in too much pain to receive manual therapy. Pain relief can allow a window of opportunity to engage in physiotherapy, which will help with treatment progression and PGP management. PGP is treatable at any stage during pregnancy. Women may also choose to engage in pilates-based exercises to improve pelvic stability ante-natal, post-natal or in preparation of getting pregnant. Should you require further guidance with these matters then please feel free to get in touch with the clinic. Renu is one of our Chartered Physiotherapists who is a qualified matwork pilates instructor, accredited by The Australian Physiotherapy and Pilates Institute, and is experienced in ante and post-natal pilates. Useful links:
Pelvic Obstetric and Gynaecological Physiotherapy http://pogp.csp.org.uk/publications/pregnancy-related-pelvic-girdle-pain-mothers-be-new-mothers The Pelvic Partnership http://pelvicpartnership.org.uk/ NHS https://www.nhs.uk/conditions/pregnancy-and-baby/pelvic-pain-pregnant-spd/ NCT https://www.nct.org.uk/pregnancy/pelvic-girdle-pain-pregnancy References: Albert, H. B. et al. 2006. Risk factors in developing pregnancy‐related pelvic girdle pain. Acta Obstetricia et Gynecologica Scandinavica 85(5), pp. 539-544. doi: 10.1080/00016340600578415 Bertuit, J. et al. 2018. Pregnancy and pelvic girdle pain: Analysis of pelvic belt on pain. Journal of Clinical Nursing 27(1-2), pp. e129-e137. doi: 10.1111/jocn.13888 Bjelland, E. K. et al. 2010. Pelvic girdle pain in pregnancy: the impact of parity. American Journal of Obstetrics and Gynecology 203(2), pp. 146.e141-146.e146. doi: 10.1016/j.ajog.2010.03.040 Mackenzie, J. et al. 2018. Women's experiences of pregnancy related pelvic girdle pain: A systematic review. Midwifery 56, pp. 102-111. doi: 10.1016/j.midw.2017.10.011 Vleeming, A. et al. 2008. European guidelines for the diagnosis and treatment of pelvic girdle pain. European Spine Journal 17(6), pp. 794-819. doi: 10.1007/s00586-008-0602-4 |
AuthorPhysioimpulse Chartered Physiotherapists Archives
June 2024
|

 RSS Feed
RSS Feed
ServicesPhysiotherapy Chiropractic Osteopathy Injection Therapy Gait Analysis/Orthotics Shockwave Therapy Bike Fit Running Analysis Sports Massage Pilates |
Get in Touch
|
©
