|
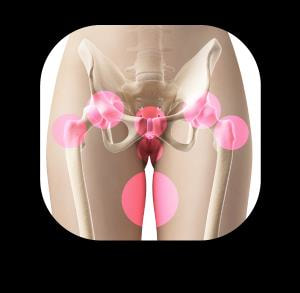
What is PGP? PGP (previously known as Symphysis Pubis Dysfunction (SPD)) affects 20-50% of all pregnant women. PGP is localised around the back of the pelvis, and described as a pain between the posterior iliac crest (the back of the pelvis) and the gluteal fold (the line where the buttock meets the thigh), particularly around the sacroiliac joint (SIJ). The pain may radiate down the back of the thigh and can also occur in conjunction with/or separately of pain in the symphysis (a cartilaginous joint located between the left and right pubic bones near the front midline of the body, just in front of the bladder). PGP can cause pain and stiffness in the pelvic joints, difficulty walking, climbing stairs and turning in bed. Common painful areas:
Pelvic girdle pain has been explained as the result of a combination increased pelvic joint mobility, mechanical strain, and altered neuromuscular control, which also affects the myofascial structures around the sacroiliac joints and the symphysis pubis. Causes Several factors have been identified as potential risk factors for PGP, including a history of previous low back pain, trauma of the back or pelvis, the number of previous pregnancies, high levels of stress, emotional distress, physically demanding work, smoking and high body mass index (BMI). This does not mean that if you have one or more of these factors you will automatically develop PGP as every women and every pregnancy is unique. However, having an understanding of potentially contributing factors can help you to take more care of yourself. Management PGP can be treated by a physiotherapist because it is a mechanical joint problem rather than a hormonal problem. Manual therapy can consist of gentle mobilisations of the pelvis and spine and soft tissue release techniques such as massage and myofascial release. Mobility exercises, postural re-education and core stability/pilates exercises are very beneficial to get your muscles working properly so that they can support your lower back and pelvis. Other management techniques include the use of a pelvic belt, which helps to reduce pelvic pain and improve comfort of pregnant women by providing gentle compression and support. Some research has shown that the narrow flexible belts allow a decrease in SIJ and overall pain; and the broader and more rigid belt can help to decrease back pain but ultimately it is important that individuals choose the style of belt that is most comfortable and offers support where they feel they need it. Women can also talk to their GP or local pharmacist about pain relieving medications. From a physiotherapy point of view, pain relief can prove very helpful in the initial instances if individuals feel that they are in too much pain to receive manual therapy. Pain relief can allow a window of opportunity to engage in physiotherapy, which will help with treatment progression and PGP management. PGP is treatable at any stage during pregnancy. Women may also choose to engage in pilates-based exercises to improve pelvic stability ante-natal, post-natal or in preparation of getting pregnant. Should you require further guidance with these matters then please feel free to get in touch with the clinic. Renu is one of our Chartered Physiotherapists who is a qualified matwork pilates instructor, accredited by The Australian Physiotherapy and Pilates Institute, and is experienced in ante and post-natal pilates. Useful links:
Pelvic Obstetric and Gynaecological Physiotherapy http://pogp.csp.org.uk/publications/pregnancy-related-pelvic-girdle-pain-mothers-be-new-mothers The Pelvic Partnership http://pelvicpartnership.org.uk/ NHS https://www.nhs.uk/conditions/pregnancy-and-baby/pelvic-pain-pregnant-spd/ NCT https://www.nct.org.uk/pregnancy/pelvic-girdle-pain-pregnancy References: Albert, H. B. et al. 2006. Risk factors in developing pregnancy‐related pelvic girdle pain. Acta Obstetricia et Gynecologica Scandinavica 85(5), pp. 539-544. doi: 10.1080/00016340600578415 Bertuit, J. et al. 2018. Pregnancy and pelvic girdle pain: Analysis of pelvic belt on pain. Journal of Clinical Nursing 27(1-2), pp. e129-e137. doi: 10.1111/jocn.13888 Bjelland, E. K. et al. 2010. Pelvic girdle pain in pregnancy: the impact of parity. American Journal of Obstetrics and Gynecology 203(2), pp. 146.e141-146.e146. doi: 10.1016/j.ajog.2010.03.040 Mackenzie, J. et al. 2018. Women's experiences of pregnancy related pelvic girdle pain: A systematic review. Midwifery 56, pp. 102-111. doi: 10.1016/j.midw.2017.10.011 Vleeming, A. et al. 2008. European guidelines for the diagnosis and treatment of pelvic girdle pain. European Spine Journal 17(6), pp. 794-819. doi: 10.1007/s00586-008-0602-4
0 Comments
Leave a Reply. |
AuthorPhysioimpulse Chartered Physiotherapists Archives
June 2024
|

 RSS Feed
RSS Feed
ServicesPhysiotherapy Chiropractic Osteopathy Injection Therapy Gait Analysis/Orthotics Shockwave Therapy Bike Fit Running Analysis Sports Massage Pilates |
Get in Touch
|
©
