Peak ACL force during jump landing in downhill skiing is less sensitive to landing height than landing position 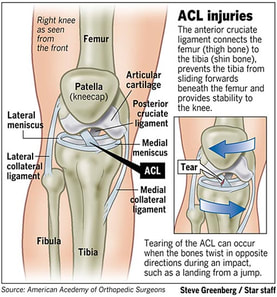 Anatomy: Anterior Cruciate Ligament (ACL) The ACL is a tough band of tissue joining the thigh bone to the shin bone at the knee joint. It runs diagonally through the inside of the knee and gives the knee joint stability. It also helps to control the back-and-forth movement of the lower leg. Methods:
 References: Heinrich D, van den Bogert AJ, Nachbauer WPeak ACL force during jump landing in downhill skiing is less sensitive to landing height than landing position Br J Sports Med Published Online First: 28 June 2018. doi: 10.1136/bjsports-2017-098964
Our Team are experts in knee rehabilitation. If you have suffered a ski accident or injury do give us a call!
1 Comment
Anterior Shoulder dislocation The shoulder complex consists of three bones: the collar bone (clavicle), the shoulder blade (scapula) and the upper arm bone (humerus). Acute anterior shoulder dislocation is an injury where the top end of the humerus is pushed out of the shoulder joint socket in a forward direction. The extent of dislocation varies from partial dislocation (subluxation) to full dislocation where the joint surfaces completely lose contact. 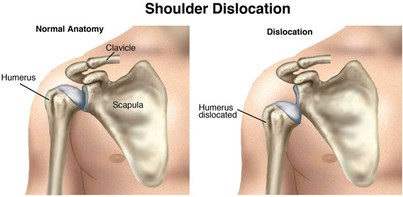 First-time dislocation generally results from trauma (injury), typically during contact sports in adolescents and younger adults. In older adults it may result from a fall from standing height. Traumatic anterior dislocation is the commonest type and accounts for >90% of all shoulder dislocations. Following a shoulder dislocation, the shoulder is generally less stable and, at times, prone to re-dislocation, especially in active young adults. Initial treatment involves putting the joint back; this is called ‘reduction’. ‘Closed reduction’ refers to cases where this is done without surgery. Afterwards, treatment is often conservative (non-surgical), and generally involves placing the injured arm in a sling or other immobilising device followed by exercises, which can be supported by a physiotherapist. The period of immobilisation varies. After reduction, and often throughout your rehabilitation, you will be re-evaluated for nerve or blood vessel injuries which can occur in traumatic cases, to ensure anything suspicious is caught early and managed accordingly. Physiotherapy Rehabilitation Conservative treatment with physiotherapy will vary depending on several factors, including, but not limited to:
To avoid repeated issues of shoulder instability or recurrent dislocations, it is imperative that the Physiotherapist guides you in returning to sport and work tasks gradually and on an individual case basis. Contact sports participants and those who perform overhead occupational work may be at higher risk for re-dislocation. Physiotherapy aims to restore functional use of the shoulder and enable the shoulder complex to have the capacity to manage the loads and demands placed upon it. Physiotherapy will focus on range of motion in the shoulder as well as regaining strength in the muscles in and around the shoulder complex, whilst also retraining the way the muscles work together (muscle patterning). ‘Hands on’ physiotherapy can also be used to address any secondary soft tissue issues that may have occurred following immobilisation. You can be supported in regaining range of motion around the shoulder joint using manual techniques such as PNF stretches and others. Here are some end stage gym exercises you can try once you have regained range of movement and basic strength. If you continue to suffer pain and weakness following a shoulder injury do give us a call and we will endeavour to help in any way possible
Central Bath Physiotherapy01225 683007References
Handoll, H.H., Hanchard, N.C., Goodchild, L.M. and Feary, J., 2006. Conservative management following closed reduction of traumatic anterior dislocation of the shoulder. Cochrane Database of Systematic Reviews. Khiami, F., Gérometta, A. and Loriaut, P., 2015. Management of recent first-time anterior shoulder dislocations. Orthopaedics & Traumatology: Surgery & Research, 101(1), pp.S51-S57. Longo, U.G., Loppini, M., Rizzello, G., Ciuffreda, M., Maffulli, N. and Denaro, V., 2014. Latarjet, Bristow, and Eden-Hybinette procedures for anterior shoulder dislocation: systematic review and quantitative synthesis of the literature. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 30(9), pp.1184-1211. Hip Adduction: Often forgotten in Hip Rehabilitation? It is common for avid exercise enthusiasts to incorporate hip strengthening exercises into their routines that focus on the hip abductors. There is seemingly a surge in popularity of exercises targeting your glutes, for instance; leg lifts, single leg work, lateral band walks. However, arguably, many people neglect the much needed companion to the abductors, the adductors. 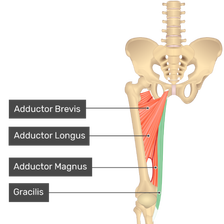 Hip Adductor Complex The adductors are a group of muscles on the inside of your thigh. The adductor magnus, adductor longus, adductor brevis, pectineus and gracilis muscles all have involvement in hip adduction (bringing your thighs together). The adductor magnus muscle has a large hip extensor muscle moment arm, which in simple terms, makes it an unappreciated hip extensor, while the other adductors are also hip flexors. Therefore, the adductors play a part in many movements of the hip Some believe that the adductor complex does not need specific, targeted exercise, as compound exercises, such as squats, sumo squats, and lunges demonstrate activation of these muscles. However, some evidence would suggest this claim was false. Of course compound exercises are integral to any strengthening exercise programme, but it is advantageous to ensure you make time to consider specific adductor muscle components. The adductor magnus is a very large and heavy muscle. It is much larger and heavier than the other adductors. By some measures it is the second largest muscle in the body after the gluteus maximus. Ignoring the adductor magnus is therefore likely to lead to a failure to maximize overall muscular hypertrophy (growth and increased size of muscle) in the lower body. Injury Risk Just like with the front and back of the leg, where there is a strength relationship between the quadriceps and hamstrings, there is also a relationship between the abductor and the adductor strength. For most, these relationships do not need to be assessed with a fine toothcomb, but these ratios are commonly used within high performance sport. Weakness in the hip adductors compared to the abductors has been shown to be a risk factor for developing groin pain in several sports, such as football and hockey. ‘don’t just sit on the hip adduction machine in the gym, seek advice on exercise from a physiotherapist or exercise professional to add variety to your programme’ During rehabilitation, it is important to remember that the adductors may be preferentially activated at different degrees of hip flexion. The adductor magnus is most active between 0 – 45 degrees, the adductor longus and gracilis are most active at 45 degrees, and the pectineus is most active at 90 degrees. Therefore, don’t just sit on the hip adduction machine in the gym, seek advice on exercise from a physiotherapist or exercise professional to add variety to your programme. Below is an example of an evidence-based exercise for strengthening your adductors. ‘Hands on’ treatment may be used in conjunction with exercise rehabilitation too. A large consensus paper, the DOHA agreement, stated that ‘Multimodal treatment including manual adductor manipulation can result in a faster return to play, but not a higher treatment success, than a partially supervised active physical training programme’. Copenhagen Adduction Exercise The Copenhagen adduction exercise (CAE) is a bodyweight, partner-assisted movement popularized by Danish researchers and sports therapists, including one of the leaders in groin injuries, Kristian Thorborg. 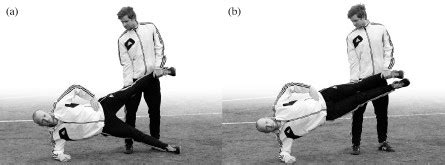 The well-known, FIFA promoted, FIFA 11+ injury prevention and warm-up programme was disseminated worldwide in 2009. More recent research has suggested adding the Copenhagen Adduction exercise to the FIFA 11+ to potentially prevent groin problems. Thorborg and colleagues also investigated other exercises using elastic bands in adductor muscle strengthening research. Here, a hip adduction movement was performed over full range of motion with 3 seconds in, 2 seconds hold, and 3 seconds out. The participants performed 3 sets of exercise with both legs during each session.  Good luck strengthening your adductors and keep active! If you have tried extensive rehab but continue to suffer just give us a call! Book Central Bath Physio01225 683007References
Harøy, J., Thorborg, K., Serner, A., Bjørkheim, A., Rolstad, L.E., Hölmich, P., Bahr, R. and Andersen, T.E., 2017. Including the copenhagen adduction exercise in the FIFA 11+ provides missing eccentric hip adduction strength effect in male soccer players: A randomized controlled trial. The American journal of sports medicine, 45(13), pp.3052-3059. Ishøi L, Sørensen CN, Kaae NM, et al. Large eccentric strength increase using the Copenhagen Adduction exercise in football: A randomized controlled trial. Scand J Med Sci Sports. 2016 Nov;26(11):1334-1342. Jackie L Whittaker, et al. (2015) Risk factors for groin injury in sport: an updated systematic review. Br J Sports Med;49,pp.803-809 Jensen, J., Hölmich, P., Bandholm, T., Zebis, M.K., Andersen, L.L. and Thorborg, K., 2012. Eccentric strengthening effect of hip-adductor training with elastic bands in soccer players: a randomised controlled trial. Br J Sports Med, pp.bjsports-2012. Weir, A., Brukner, P., Delahunt, E., Ekstrand, J., Griffin, D., Khan, K.M., Lovell, G., Meyers, W.C., Muschaweck, U., Orchard, J. and Paajanen, H., 2015. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br J Sports Med, 49(12), pp.768-774. Cycling ScienceOver the past few years, the popularity of recreational road cycling has significantly increased. I should know as I finally got on a road bike this year and absolutely love it! Cycling is low impact and non-weight bearing which results in fewer injuries when compared to other sports, and this may play a role in the attractiveness of cycling at any age. The sport includes long-distance endurance cycling and high intensity efforts when sprinting or hill climbing. As a result, cyclists need to train both aerobically (“with oxygen”) and anaerobically (“without oxygen”). The main energy currency used all over the body is Adenosine triphosphate (ATP). ATP is broken down to adenosine diphosphate (ADP) which releases energy. ATP is produced along an energy continuum involving three key energy systems: the phosphocreatine (ATP-PC) system, which produces ATP during extremely high-intensity activity lasting up to 30-seconds; anaerobic glycolysis which produces ATP during high-intensity activities from 6-120-seconds; and aerobic metabolism which produces ATP during low-intensity activities, from 120 seconds onwards. Note that there is an overlap in the activation of the energy systems meaning that ATP production occurs with at least two energy systems at one time. Given that road cyclists require both anaerobic and aerobic power, all three of these systems need to be trained. Interestingly, analysis of cycling grand tours such as The Tour de France, reveal that cyclists can spend approximately 20-minutes per day over the individual anaerobic threshold, and when on hilly stages they are riding at high intensities of between 70-90% of their VO2max (the measurement of the maximum amount of oxygen a person can utilise during intense exercise), hence this group of athletes need to be able to tolerate high workloads over long periods of time. They also need to be able to produce brief episodes of high-power outputs, for example when steep climbing or sprinting at the race finish. The pedal cycle consists of the power phase and the recovery phase. During the pushing action of the power phase, the hip and knee joints extend at the same time powered by the hip extensors (gluteal and hamstring muscles) to initiate the movement and the knee extensors (quadriceps muscles) to move the crank forward, and then together they work to gain momentum on the crank to apply a substantial driving force onto the pedals. The plantarflexors of the foot (the calf muscles) contract for a short period following this. During the recovery (upstroke) phase the tibialis anterior engages to dorsiflex the ankle, and the knee and hip flexors contract to draw the pedal back to the top centre of the crank cycle. Overall the quadriceps contraction is almost twice that of the hamstrings. Cycling also requires core, upper back, and upper limb strength to maintain good posture on the bike for prolonged periods. 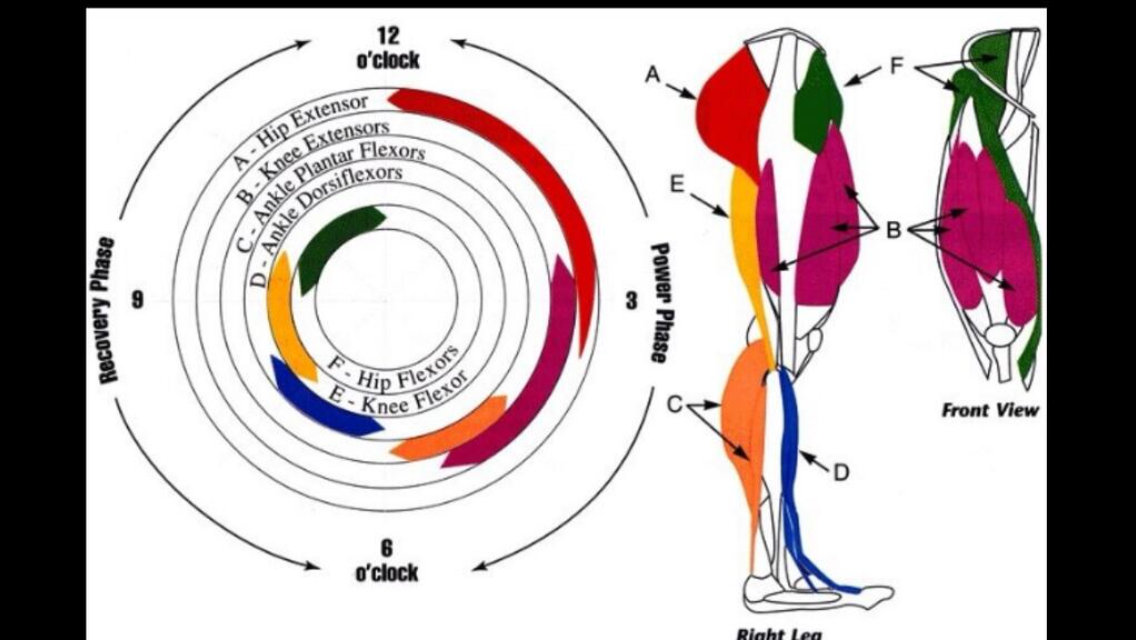 Bath Cycling Physio 01225 683007Aerobic training involves longer duration rides at 60-80% maximum effort. Aside from cardiovascular benefits, this type of training develops type I slow-twitch muscle fibre types, which are very resistant to fatigue. Strength training is advocated because of potential improvements in speed, anaerobic capacity and movement economy, and in postponing the effects of fatigue. Strength training is an anaerobic training modality which can lead to improvements in both the ATP-PC and anaerobic systems. A further benefit of strength training is that it increases the size and strength of muscles fibres, particularly type II fast-twitch fibres. Type II muscle fibres use anaerobic metabolism and provide short bursts of power. These adaptations can result in higher peak power output during cycling and thus an improved power to weight ratio, which is advantageous to cycling performance. High-intensity training for 30-40 seconds followed by a recovery period can also help to influence the ATP-PC system. The pedalling motion and power during cycling is created by the cyclists’ legs, however a strong core is important, particularly when riders are in the saddle for many hours. Many postural muscles contain type I muscle fibres as they need to have endurance capabilities, and core stability training can help to strengthen this group of muscles. Core stability has been described as three co-dependent subsystems: passive (skeleton), active (muscles), and neural control (nerves). Constant communication between all subsystems is required for the maintenance of stability, and exercise programs should aim to incorporate these different aspects. Sports medicine literature describes core stability as the neuromuscular control required to allow the “production, transfer, and control of force and motion to distal segments of the kinetic chain”. In a cyclist, a stable core could help to prevent energy loss by reducing trunk rotation and shoulder movements. Improved core stability also increases pelvic stability and balance in the saddle, which in turn helps to ensure sound lower limb alignment and greater force transmission from the torso to the legs. Core strength and stability also allows for highly coordinated muscle activation patterns to change continually, depending on the demands of the task at hand. Core stability exercises should be aimed at strengthening the scapula-thoracic region and the abdominal, lumbar spine and hip muscles. Our clinic can help you with core stability training, strength and conditioning training, bike fits to ensure optimum positioning on the bike, as well as assistance with any cycling musculoskeletal injuries or problems. Stay safe and happy cycling! Book online
|

 |
|
If these simple tips do not rectify your problem our team here at Physioimpulse will be able to help you on your way to recovery with a full assesment, hands on treatment and a tailor made exercise programme. Please call if you would like an appointment: 01225 683007 or you can simply book online.
Central Bath Physiotherapy 01225 683007
Sacroiliac Joint (SIJ) Pain
SIJ pain can be caused by twisting at an awkward angle (usually combined with bending forward), leaning to one side when sat on the sofa for a long period of time or missing a step when descending the stairs. Anyone can suffer from this common condition, including desk workers, athletes or during pregnancy when a hormone called relaxin causes the pelvic ligaments to relax.
In many cases, this joint when restricted does not cause pain initially but over time muscle tension can build after shifting our weight to the other side to compensate for the lack of movement in the joint that has now become irritated. This can lead to irritation of the sciatic nerve, leading to pain radiating down the legs and around the hips.


Bath Chiropractic 01225 683007
Watch this video explaining how a manipulation is carried out to the lumbar spine or SIJ. Below that is a great strengthening exercise for the gluts to support the SIJ.
Patella femoral joint pain (PFJP) commonly known as Runner's Knee

Risk factors
- Activities that frequently aggravate symptoms include running (particularly longer runs, downhill running or running on cambered surfaces)
- walking (particularly up and down stairs or hills)
- Muscular tightness/weakness (particularly quads, hamstrings, TFL core and glutes).
- Excessive or inappropriate training load (mileage, intensity)
- Abnormal biomechanics or poor running technique.
- Recent changes or inappropriate footwear or surfaces
Signs and symptoms
Patients with PFJ pain experience pain on the anterior aspect (front) of the knee. Patients usually experience an ache that may increase to a sharper pain with activity. Pain is typically experienced during activities that bend or straighten the knee repetitively particularly whilst weight bearing, such as running or squatting in the gym. Pain may be worse first thing in the morning or following activity (once the body has cooled down). This may be associated with knee stiffness and can sometimes cause the patient to limp.
Clinical signs
Patients with PFJP typically experience pain when firmly touching the distal aspect of the patella and the patellar tendon and also mobilising the patella. In more severe cases, swelling may be present at the anterior aspect of the knee along with an associated grinding sound when bending or straightening the knee. Occasionally, patients may also experience episodes of the knee giving way or collapsing due to pain.
Investigations
A thorough subjective and objective examination from a physiotherapist is sufficient to diagnose PFJP. Investigations such as an ultrasound or MRI may be used to assist with diagnosis.
Management options
Physiotherapy treatment for PFJ is vital to speed up the recovery process, ensure an optimal outcome and reduce the likelihood of recurrence. Treatment options include:
- soft tissue massage (particularly to the quads)
- mobilisation of the patella
- dry needling
- electrotherapy
- ice or heat treatment
- progressive exercises to improve flexibility, strength and balance
- activity modification advice
- biomechanical correction (see our biomechanics page)
- anti-inflammatory advice
- Clinical Pilates and core stability exercises
- footwear advice
Central Bath Physiotherapy
- The average office worker is likely to spend 65,000 hours in a office chair from leaving full time education until retirement .
- 33% of long term sickness is due to work related musculoskeletal disorders such as back and neck pain.
- 31 million working days are lost in UK (approx £100billion/year) due to MSK disorders, neck and back pain.
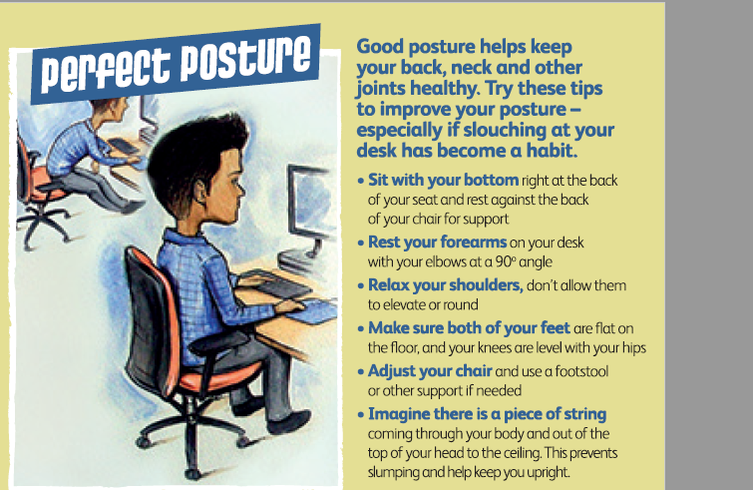
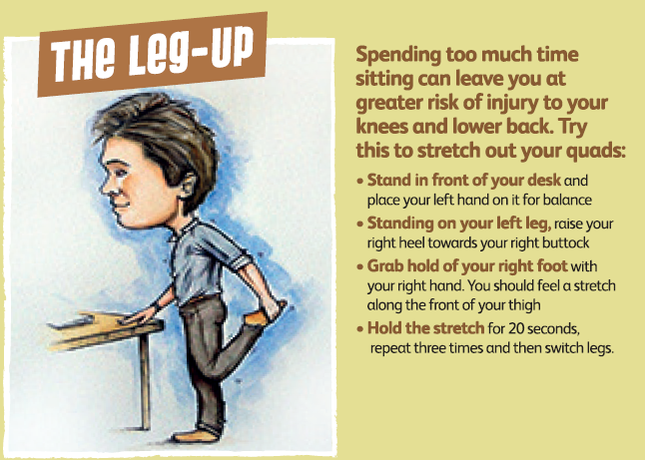
The Chartered Society of Physiotherapy have come up with some top tips to help with your desk environment:
- Moving more throughout the day can help keep your weight at a healthy level and limit your chances of developing a number of serious illnesses.
- UK exercise guidelines recommends adults aged 19-64 take at least 150 minutes of moderate to vigorous intensity physical activity each week, aiming to be active every day.
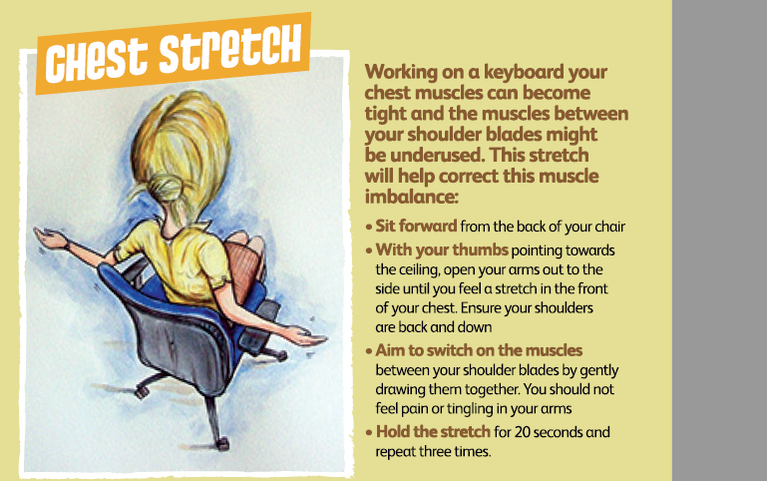
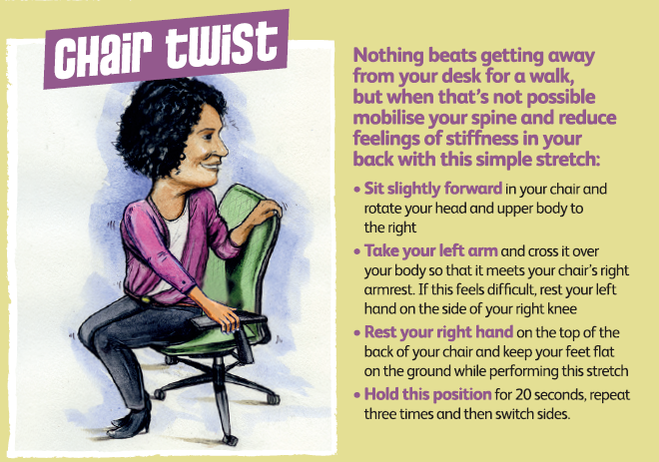
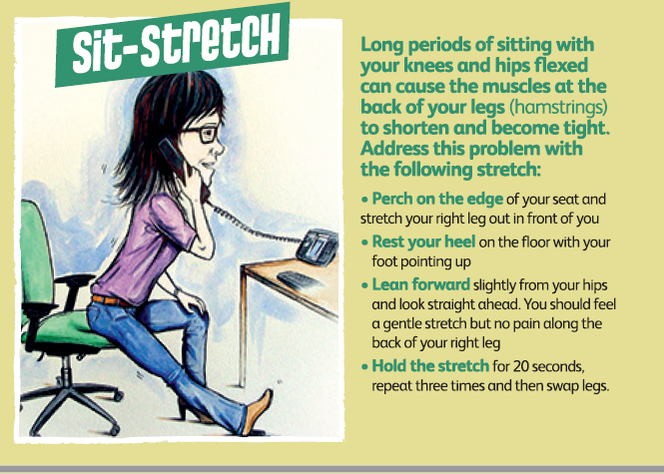
These simple stretches can help ease the aches and pains associated with sitting for long periods combined with regular physical activity:
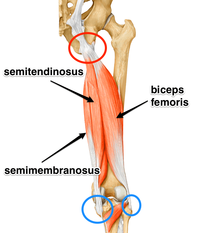
Acute hamstring injuries are common and generally present with localised pain following rapid acceleration or deceleration movements, such as when sprinting, and frequently occur in sports such as football, skiing, and hockey, to name a few. Acute injuries can also occur when the muscle is stretched too far Whereas chronic/persistent hamstring injuries present with a stealthy onset of unrelenting pain made worse with sports activities and sitting – often found in runners.
It is very important to treat and rehabilitate hamstring injuries correctly; incorrect or improper healing makes re-injury more likely. For the first 3 to 5 days (in the acute phase), the general consensus is to control swelling, pain and bleeding. The POLICE method is often used. POLICE stands for Protection, Optimal Loading, Ice, Compression and Elevation.
Following this acute phase, there was previously some ambiguity among treatment protocols until the introduction of Askling and colleagues’ 2013 research. In this paper, Carl Askling and colleagues used 75 elite Swedish football players to compare two different hamstring rehabilitation protocols called the C-Protocol and L-Protocol. They then assessed outcomes of return to play and re-injury. The L-Protocol focused on eccentric loading of the hamstrings while the C-protocol consisted of conventional hamstring rehabilitation exercises. Participants in the L-protocol (outlined below) were able to return to sport significantly faster than those in the conventional group (mean 28 days vs 52 days). Their research into which protocol was best for chronic injuries was inconclusive, but the researchers were able to surmise that rehabilitation protocols consisting of eccentric exercises are more effective in returning athletes to their sports following hamstring injury.
Additionally, it is recommended that hamstring injury rehabilitation protocols should be preferentially based on strength and flexibility exercises that primarily involve exercises with high loads at long muscle–tendon lengths.
The L- Protocol Exercises
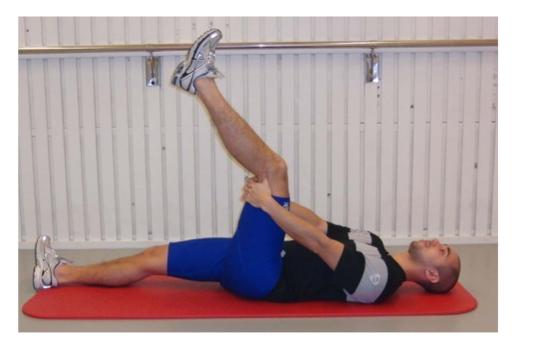
- L1 - The Extender
- The athlete lays in the position shown then slowly extends the knee
- The knee is straightened as much as possible, not through pain
- Three sets of 12 repetitions, twice per day
- L2 - The Diver
- The athlete stands on the injured leg in the position shown. Both hands are then reached forward slowly whilst the leg is reached backwards
- Three sets of 6 repetitions are performed every other day at a slow tempo

- L3 - The Glider
- The athlete starts with one hand holding onto a railing or support and 90% of the weight on the injured leg with a slight knee bend
- The uninjured leg is then glided backwards, stopping before pain on the injured leg
- The arms are then used to return the athlete to the starting position
- Three sets of 4 repetitions every third day
- Progress this exercise by increasing the range of motion and speed at which it is performed

Good luck and keep active!
Chris, PhysioImpulse
Author
Physioimpulse Chartered Physiotherapists
Archives
April 2024
February 2024
January 2024
October 2023
May 2023
February 2023
December 2022
August 2021
July 2021
February 2021
January 2021
July 2020
February 2020
August 2019
July 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
December 2017
May 2017
February 2017
January 2017
November 2016
June 2016
April 2016
February 2016
January 2016
December 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
February 2015
January 2015
September 2014
August 2014
 RSS Feed
RSS Feed
