Anterior Shoulder dislocation The shoulder complex consists of three bones: the collar bone (clavicle), the shoulder blade (scapula) and the upper arm bone (humerus). Acute anterior shoulder dislocation is an injury where the top end of the humerus is pushed out of the shoulder joint socket in a forward direction. The extent of dislocation varies from partial dislocation (subluxation) to full dislocation where the joint surfaces completely lose contact. 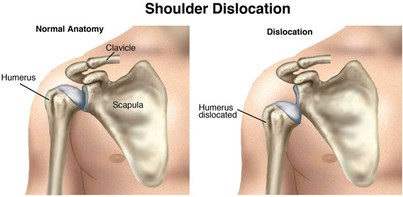 First-time dislocation generally results from trauma (injury), typically during contact sports in adolescents and younger adults. In older adults it may result from a fall from standing height. Traumatic anterior dislocation is the commonest type and accounts for >90% of all shoulder dislocations. Following a shoulder dislocation, the shoulder is generally less stable and, at times, prone to re-dislocation, especially in active young adults. Initial treatment involves putting the joint back; this is called ‘reduction’. ‘Closed reduction’ refers to cases where this is done without surgery. Afterwards, treatment is often conservative (non-surgical), and generally involves placing the injured arm in a sling or other immobilising device followed by exercises, which can be supported by a physiotherapist. The period of immobilisation varies. After reduction, and often throughout your rehabilitation, you will be re-evaluated for nerve or blood vessel injuries which can occur in traumatic cases, to ensure anything suspicious is caught early and managed accordingly. Physiotherapy Rehabilitation Conservative treatment with physiotherapy will vary depending on several factors, including, but not limited to:
To avoid repeated issues of shoulder instability or recurrent dislocations, it is imperative that the Physiotherapist guides you in returning to sport and work tasks gradually and on an individual case basis. Contact sports participants and those who perform overhead occupational work may be at higher risk for re-dislocation. Physiotherapy aims to restore functional use of the shoulder and enable the shoulder complex to have the capacity to manage the loads and demands placed upon it. Physiotherapy will focus on range of motion in the shoulder as well as regaining strength in the muscles in and around the shoulder complex, whilst also retraining the way the muscles work together (muscle patterning). ‘Hands on’ physiotherapy can also be used to address any secondary soft tissue issues that may have occurred following immobilisation. You can be supported in regaining range of motion around the shoulder joint using manual techniques such as PNF stretches and others. Here are some end stage gym exercises you can try once you have regained range of movement and basic strength. If you continue to suffer pain and weakness following a shoulder injury do give us a call and we will endeavour to help in any way possible
Central Bath Physiotherapy01225 683007References
Handoll, H.H., Hanchard, N.C., Goodchild, L.M. and Feary, J., 2006. Conservative management following closed reduction of traumatic anterior dislocation of the shoulder. Cochrane Database of Systematic Reviews. Khiami, F., Gérometta, A. and Loriaut, P., 2015. Management of recent first-time anterior shoulder dislocations. Orthopaedics & Traumatology: Surgery & Research, 101(1), pp.S51-S57. Longo, U.G., Loppini, M., Rizzello, G., Ciuffreda, M., Maffulli, N. and Denaro, V., 2014. Latarjet, Bristow, and Eden-Hybinette procedures for anterior shoulder dislocation: systematic review and quantitative synthesis of the literature. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 30(9), pp.1184-1211.
0 Comments
Leave a Reply. |
AuthorPhysioimpulse Chartered Physiotherapists Archives
June 2024
|
 RSS Feed
RSS Feed
ServicesPhysiotherapy Chiropractic Osteopathy Injection Therapy Gait Analysis/Orthotics Shockwave Therapy Bike Fit Running Analysis Sports Massage Pilates |
Get in Touch
|
©
