 At Physioimpulse we provide therapeutic injections in conjunction with Physiotherapy treatment to optimise recovery from injury and reduce pain in degenerative conditions such as Osteoarthritis.
Injection therapy can benefit the following conditions:
Injections are performed by our Clinical Specialist Physiotherapist Matt Shepherd who has undertaken extensive Post Graduate training in order to carry out injections at our Bath Physiotherapy Clinics. We are receiving some great feedback on the pain relieving effects of our Ostenil Plus injections which enable people to return to their normal activities of daily living with greatly reduced reports of pain. The study below outlines the benefits of these injections in delaying the need for major knee surgery If you would like to know more about these injections read our Injection Therapy page or email [email protected] 01225 683007 The use of intra-articular hyaluronic acid (HA) injections in patients with osteoarthritis (OA) of the knee has shown efficacy in delaying total knee replacement (TKR) surgery in a recent retrospective, longitudinal study published in PLoS One. The investigators sought to compare the delay from diagnosis to TKR surgery in patients with knee OA who received intra-articular HA injections vs those who did not. All patients studied were treated in France between 2006 and 2013. A second objective of the study was to compare direct medical costs associated with ambulatory care between the 2 groups. A total of 14,782 patients were treated for knee OA (ages ≥50 years; mean age, 68±10 years; 67% women). Annual incidence rates of knee OA were estimated to be 0.52% in women and 0.92% in men. Of the 14,782 patients, 1662 individuals (11.2%) underwent TKR surgery before the end of 2013. At each point evaluated, restricted mean survival time without TKR surgery was higher in the HA treatment vs no injection group (from 51 days at 1 year after diagnosis to 217 days at 7.5 years, respectively; P <.001). This is the first retrospective longitudinal study involving patients with knee OA that used medico-administrative databases in France. The investigators concluded that “the results support the effectiveness of [HA] injections in delaying [TKR] surgery. Reference Delbarre A, Amor B, Bardoulat I, et al. Do intra-articular hyaluronic acid injections delay total knee replacement in patients with osteoarthritis – A Cox model analysis. PLoS One. 2017;12(11):e0187227.
0 Comments
Biomechanics Assessment and Orthotics In BathOur Biomechanics expert Stuart specialises in the assessment of foot and lower limb pain such as
An appointment with Stuart will involve not only an assessment of the mobility in your feet in lying and standing but also a gait analysis will be undertaken with the use of the latest computerised technology in a pressure plate. This allows us to get a clear idea of what happens to your foot as you walk or what we call the gait cycle. 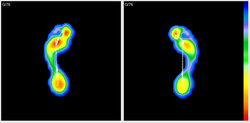 Here is an image from a recent assessment. What do we see With areas of blue showing low pressure and conversely red high pressure, we see reduced outside (lateral) contact on the right side as an indication of early pronation during the gait cycle. The line you see in the middle shows the transfer of force during the gait cycle and with a flat initial curve further towards the arch we again see evidence of early pronation on the right comparative to the left. So what do we do about it? In this instance we casted bespoke orthotics for a runner who had recurrent right sided 'shin splints' (or tibialis posterior tendinopathy) related to the overactivity of the muscle which was attempting to exert control over the early pronation but with a reduced mechanical advantage. 100% success with this now happy runner!biomechanics service click here For more information on our biomechanics service click here Bath Orthotics and PhysiotherapyAt this time of year we have a deluge of running enthusiasts limping in to our Physioimpulse clinic rooms pleading to be healed in time for the Bath Half or the next big Marathon. We understand the pressures involved in completing the run for that special charity close to your heart or to knock spots off last year’s PB, so we have produced this guide to help you stay injury free! 5 Common running Injuries 1 Runner's Knee/Anterior Knee Pain Patellofemoral pain syndrome (PFPS), or "runner's knee," is the irritation of tissue on the underside of the patella (knee cap). PFPS typically flares up during or after long runs, after extended periods of sitting, or while descending hills and stairs. Anyone with biomechanical factors that put extra load on the knee such as quads shortening or gluts (gluteal or buttock muscles) weakness is vulnerable to PFPS. Changes in training surfaces/frequency/intensity or running style can also put you at risk. 2 “Shin splints” Because we like fancy words at Physioimpulse, we call this condition Medial Tibial Stress Syndrome (MTSS). Basically it is when too much stress/load is placed through the inside of the shin muscles, tendons or bone resulting in a nasty shin pain with each step. Footwear and “overpronation” is often blamed for this condition but we find that training history, running form and muscle control are more likely culprits. 3 Achilles Tendinopathy /pain The Achilles tendon connects the two major calf muscles to the back of the heel. Under too much stress, the tendon properties alter which may result in debilitating pain in the heel or just above. Runners who dramatically increase training, particularly hills and speed work or have tight weak calves are susceptible. 4. Plantar Fasciitis A sharp, painful sensation at the base of the heel, often described as like having a stone in your shoe. At its worse when you first step out of bed this pesky injury can halt your training plan in its tracks. Overtraining and improper or worn-out footwear can cause pain in your heel, but the root of the problem lies in tight and weakened muscles in the foot. If your feet are weak, the heel takes on an excessive load and can’t handle your gruelling training regime. 5. “ITB Syndrome” Symptoms of ITB (Iliotibial band) syndrome consist of pain on the outside of the knee, more specifically at or around the lateral epicondyle of the femur (the bony bit on the outside of the knee). It comes on at a certain time into a run and gradually gets worse until often you have to stop. After a period of rest the pain may go only to return when running starts again. The pain is normally aggravated by running, particularly downhill. People usually go straight to foam rolling or massage for this injury but an additional glutes strengthening programme with gait retraining will often be far more successful. Injury Treatment and Prevention Injuries are always multi-factorial and their management multi-modal so we will break this down in to 5 parts 1. Training Programmes/Progression 2. Running Technique and footwear 3. Strength and Conditioning 4. Stretching 5. Physiotherapy Training Programmes/Progression We love treating your aches and pains to help you get back to pounding the pavements but prevention is always better than cure so a graded training programme is essential when partaking in a race or increasing fitness. There is an age old injury mantra in physiotherapy which continues to hold true – too MUCH, too SOON, too OFTEN will overload your normally robust body and may result in injury. If you do: Too MUCH - E.G. Running 10 miles when you have only covered 1 previously. Too SOON - E.G. Enthusiasm leads you to running that 10 miles in week 1 of training. Too OFTEN - E.G. You run that 10 miles 5 times in a week as the race is only a month away and you spent Xmas in front of the fire rather than training. You will predispose yourself to the injuries we listed previously and more. Thankfully the human body is a fantastic piece of kit and will allow us to perform amazing feats so long as we prepare it adequately. It’s all about appropriate loading of tissue at the right time. If you gradually add load (increase training) at a responsible rate the cells and tissues of your body will adapt to the load and strengthen for your next training session. This will reduce the chances of you needing our help! Luckily a host of excellent training programmes with graded progression are available to help you complete your race and stay injury free. Here is a link to a couple of programmes written by running experts for the Bristol 10k/Half http://www.runbristol.com/Blog/training-plans Running Technique and Footwear Running technique is a tricky one as without tuition you will already have developed your own unique running style. We generally say that if you are enjoying your running and it feels easy then you are doing something right. If however your running feels laboured and you are picking up the odd niggle or a lot of injuries then it is likely your running technique could be improved. When we undertake our running analysis the most common finding is that people tend to brake slightly when they land, meaning that despite a good landing foot position, the impact through the heel/foot is increased because the hip position is sub-optimal. So how do we go about changing this? Well it’s hard to know for sure whether this is definitely you but it wouldn’t hurt to undertake a few hopping drills and show your body what it feels like to land with your hip over your foot at initial contact. Why not try it now? Stand on one leg, lean forward until you are able to fall forward and save yourself by hopping forward. Try repeating this for 10 seconds each side just prior to going running or a couple of times on your rest days and see how you feel. Footwear is also key as we often find a biomechanical component to these lower limb problems. The two main things you find in a running shoe is that it either does or doesn’t have an arch support (look at the underside of the shoe and see if there is an extra piece of plastic or a bar in the middle near the arch of your foot) which firstly adds extra support and secondly a motion control adaptation, which is useful if you do land/strike with your heel. Although it’s hard to know for sure without analysing an individual style if you take the time to run up and down the street outside the running shop then you’ll get an idea of comfort and all good running shops will encourage you to do this. A motion control device (dual density heel, normally with a firmer inner part to reduce the amount and the rate at which you pronate or how quick and how much your foot rolls in wards and flattens) is helpful if you tend to strike with your heel but superfluous if you have a mid-foot landing position. Obviously it’s hard to tell but if you are buying a pair of running shoes with motion control and it does transpire you have a good landing position then it won’t necessarily lead to any problems, it’s just like having cruise control on your car and never using it. It may also help with longer runs when you start to fatigue and who knows it may make all the difference if and when you hit the wall! Strength and Conditioning In clinic we consistently find injured runners present with impaired strength, power, balance or muscular control. This correlates with a host of recent research which points to reduced strength as one of the major risk factors of injury. When training for an event it is easy to get caught up in the need to carry out x number of miles in x number of weeks without consideration of any other training needs, particularly strength and conditioning. As discussed previously we need to load tissues appropriately and including some strength work in your weekly plan is a great way to prepare those tissues and also add variety to your training. Pictured below is Mo Farah working on strength and stability  If a finely tuned Olympic athlete needs to work on this it makes sense that we should also devote some time to strength and conditioning. There are many way to work at strength and conditioning and we have some great exercises on our website HERE A good starting point is to work on squats, lunges, and single leg dip variations focussing on balance, form and control. Research has found an association between dynamic knee valgus (the knees coming together) and increased stress load through the joints and muscles of the leg. It is therefore important to work on “alignment” throughout your exercises as depicted below. Stretching There has been a lot of negative press recently, portraying certain stretching as harmful and strength inhibiting. These sensationalist headlines are generally based on a few cherry picked studies that cannot be applied to the population as a whole. In clinic we find stretching a useful tool to increase or restore range of movement as part of a multi-modal physiotherapy treatment programme. We use and recommend a combination of dynamic and static stretches depending on the goal of the individual patient. Runners tend to develop restrictions in particular movement patterns due to the repetitive nature of the sport and stretches are a useful way to retain range of movement whilst working at strength and control. Yoga enthusiasts will be familiar with the sun salutation sequence pictured below. Usually we would recommend multi-planar stretching (stretching in all different directions) but the sequence below is often a priceless addition to a runners training programme. Give it a try! Physiotherapy Treatment Physiotherapy intervention can take many approaches ranging from hands on manual therapy and the provision of therapeutic home exercises to the use of acupuncture and electrotherapy and taping. However by far the approach we find most useful with running related injuries is the former. The main aims of treatment are to enable you to run pain free or more efficiently by treating the direct cause of your symptoms and to then teach you exercises to help maintain those beneficial effects. However it’s also just as important to treat the underlying causes of injury which are often associated with a variety of factors such as muscle imbalances around your hip and certain postural types. Whereas self-help is key, most people find it more effective to build on improvements made with ‘hands on’ physiotherapy which creates a ‘window of opportunity’ to both counter symptoms and their contributing factors. Please do not hesitate in getting in contact if you have any questions and if you are running Bristol to Bath or any other upcoming event, good luck! Physioimpulse.
Whether you have sustained a recent injury or are struggling with a long term issue we aim
to provide individually tailored manual therapy sessions and sports specific exercise programs to not only prevent recurrence, but to enhance sporting potential. For this we follow a simple three step program, assessment, treatment and prevention: Assessment is key: we will assess you as an individual to highlight any imbalances or misalignments and tailor rehab for your specific sport. We will assess the nature of your sport and uncover the potential causes of injury. Tailored Treatment: Using a variety of manual treatment techniques we aim to treat the acute symptoms, reduce swelling and restore function. Such techniques include soft tissue massage, joint mobilisation, manipulation, taping, acupuncture and electrotherapy. Prevention: Using the most up to date and valid methods we will implement functional strengthening programs and re-education of motor patterns to not only reach but exceed your previous fitness level. Building on our assessment, using the ergonomics of your sport we will aim to introduce optimal movement patterns and efficiencies to alleviate the symptoms of inappropriate repetitive strain with the ultimate aim of preventing reoccurrence If you are struggling with sports injury book an appointment without delay and we will strive to get you back on the field! This videos shows our top sports physio running through graded strengthening after a hamstring injury What is Tendinopathy?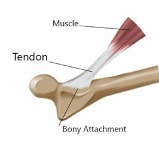
 How do we manage tendinopathy?
 Addittional treatment
Bath Physio & Shockwave
|



|
|
|
If you have any further questions, or would like to find out if chiropractic care is a suitable
form of treatment for you, give us a call on 01225 683007.
Bath Chiropractic
A chiropractic adjustment, also known as spinal manipulation when applied to the neck or
back, will vary in nature depending on the area of the body being treated.
When treating the neck, spinal manipulation is a process whereby your chiropractor will
apply a quick but gentle movement to your head and/or neck, this may or may not produce
an audible clicking sensation known as an audible release.
Adjustments throughout the midback and low back are achieved through a quick and firm
impulse applied to the area, similarly to neck adjustments this may or may not produce an
audible clicking.
Adjustments can also be applied to a number of joints in the arms or legs, whereby this
similar quick and firm impulse can be utilised to manage pain in these regions.
The adjustment itself isn’t painful, although some individuals do experience a muscular
pulling sensation in surrounding regions to the adjustment site whilst your practitioner is
getting you into position prior to performing an adjustment. This is common and nothing to
be concerned about, although important that you let your clinician know if you do
experience this, so they can change your positioning to ensure your comfort throughout.
If you and your practitioner have deemed chiropractic adjustments as an appropriate form
of management, they could help you gain benefits such as:
- Decreasing pain within your joints and surrounding muscles
- Increasing your range of movement of your neck or back, to reduce sensations ofstiffness and restricted movement
- Some individuals have been shown to obtain improved posture with a tailoredchiropractic treatment plan
- Some studies have shown adjustments to help improve athletic performance
- Many also find that chiropractic adjustments reduce their need to rely on pain medications
or from home, facilitating recovery
What common conditions can a chiropractor help treat?
Chiropractors treat conditions or pain arising from the musculoskeletal and peripheral
nervous system, meaning they treat the joints, muscles, tendons, ligaments and nerves
throughout the whole body. This means chiropractors can treat a vast variety of conditions
which involve these areas of the body, however common conditions that chiropractors
regularly see and treat in clinic include:
- Neck pain
- Headaches and migraines
- Pain in the arms or associated joints
- Midback pain
- Low back pain
- Sciatica
- Leg pain or pain in the joints of the legs or feet
- Sports injuries
to massage and soft tissue release techniques, there’s a broad spectrum of conditions
they’re able to help you manage.
Bath Chiropractic 01225 683007
References for above –
Pain management = https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6112063/
(Mann et al,2018),
https://www.nice.org.uk/guidance/ng59/chapter/Recommendations
(NICE, 2016),
Evidence based evaluation & management of common spinal conditions: A guide for the
manual practitioner (Browning, 2021). Orthopaedic Conditions (Vizniak, 2016).
Increasing ROM - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3487906/systematic
review by (Millian et al, 2012).
Posture -https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5574330/
Athletic performance -
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6555009/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3154064/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843672/
– Evidence based evaluation & management of common spinal
conditions: A guide for the manual practitioner (Browning, 2021) and NICE guidelines
(2016).
Sciatica is a term used to describe pain which starts in the low back or buttock and travels
down the leg into the foot. It occurs when a large nerve which travels from the low back
into the foot, called the sciatic nerve, is compressed or irritated. This compression can come
from a variety of sources in the back and can be identified by seeking help from one of our experienced Bath Chiropractor and Physiotherapy team.
It’s also important to note that there are a variety of causes of low back, buttock and leg
pain other than sciatica. If you’re unsure of what’s causing your pain, our clinicians at
Physioimpulse can help in identifying the cause of your discomfort.
What symptoms could suggest sciatica?
- Pain which originates in the low back or buttock and travels into the foot
- Numbness or tingling in the leg or foot
- Loss of muscle strength in the lower part of the leg or foot
How will my Bath Chiropractor diagnose sciatica?
Typically, a chiropractor will be able to determine the presence of sciatica through your
symptoms and testing of the nerves, joints and muscles in the lower limb. These tests are
non-invasive, and your clinician will explain what they’re doing as they go. In some cases a
clinician may decide to refer you for a scan, however recent evidence has proved that a scan
isn’t always essential for an accurate diagnosis of sciatica.
How can sciatica be treated in clinic?
- Manual therapy techniques administered by your chiropractor or physiotherapist to reduce discomfort and stiffness
- Tailored advice on how you can adapt your activities of daily living to reduce theimpact sciatica has on your daily life
- Exercise rehabilitation to support your body’s recovery
- Education on the associated risk factors to aid recovery and reduce the risk of reoccurrence
What can I do in the meantime to reduce my chance of developing back pain and sciatica?
The latest evidence tells us that keeping active, eating a varied and balanced diet to
promote overall health, and abstaining from smoking are some of the key factors in
reducing our chances of suffering with low back pain or sciatica.
Interestingly, we’ve also learnt through research that walking appears to be the gold
standard exercise type in preventing and treating generalised low back pain. However, if
you’re unsure of what other types of exercise can help treat low back pain or sciatica, or
have any additional questions or concerns with your low back pain, give us a call and one of
our clinician’s will happily help guide you.
Bath Chiropractic
01225 683007
The impact of tennis injuries can be reduced by careful management of swelling, protection of the injured structures from further injury, and by enlisting the support of one of our Bath chartered physiotherapist or our sports chiropractor or osteopath.
Collateral tissue damage can be minimised by following the POLICE or PRICE guidelines, standing for protection, optimal loading/rest, ice, compression and elevation.
Current evidence as published by the Association of Chartered Physiotherapists in Sports & Exercise Medicine (ACPSEM) should be followed to minimise collateral tissue damage.
- Protection: splints, taping, crutches, modifying activity
- Optimal loading/rest: load the tissues relative to their state of injury and repair
- Ice: cold compress, cold water immersion
- Compression: strapping, compression garments
- Elevation: place injured part higher than the heart
Anti-inflammatories are not recommended in the first 5-7 days after injury, as inflammation is the body’s way of healing.
Swelling needs to be managed, but stopping inflammation from occurring at all is not advised.
A chartered physio will perform a thorough assessment to evaluate how well joints and muscles are functioning.
In addition the physio will assess muscle power, strength and endurance as well as balance, co-ordination and joint position awareness.
Injured players will be guided from the initial phase after the injury to the end phase of return-to-play testing.
It is important to rehabilitate fully after any injury as failure to do so often leads to re-injury often resulting in a longer period off play.
Rotator cuff tear
What is it? The rotator muscle complex provides stability and controls movement of the shoulder joint. Tears may be due to overuse or acute trauma.
How does physiotherapy treat rotator cuff tears? Acute soft tissue management as evidenced by the PRICE guidelines (above) should be undertaken to reduce secondary damage from swelling. Simple painkillers may be taken but anti-inflammatories should be avoided at this stage.
Once again a thorough examination will guide the treatment plan which may include mobilisations, soft tissue techniques, taping, acupuncture and other physiotherapy modalities.
The physiotherapist will write a graded rehabilitation plan including return to play testing.
Shoulder injuries: famous tennis examples Maria Sharapova had surgery to repair two rotator cuff tears in 2008 and has since suffered other problems with her shoulder.
Lower back pain
What is it?This is very common among tennis players because of the repetitive nature of the game and the demands of the strokes, especially serving. Acute pain may result from a sudden stretch or fall or ongoing ache may be experienced.
Physical conditioning is very important to minimise the risk of low back pain in recreational as well as elite tennis players.
How does physiotherapy treat lower back pain?A full assessment of movement control, flexibility, strength and endurance will guide the treatment and rehabilitation plans.
Our Team may use hands-on techniques for joints and soft-tissues, taping, acupuncture, exercise prescription, and practical advice.
Back injuries: famous tennis examples Roger Federer has suffered long-term issues with his back that he manages with core strength training and by playing fewer tournaments, while Andy Murray underwent surgery last year to address a long-standing problem.
Wrist sprain
What is it? The wrist contains many small joints and ligaments and has a cartilage structure, TFCC, like the knee meniscus, which can be injured.
How does physiotherapy treat wrist sprain?The physiotherapist will follow the PRICE guidelines (above) and may protect the joint with a splint or strapping. A full examination will be undertaken to determine which structures are involved.
A graded exercise program, including return to play testing, will be undertaken alongside hands-on treatments.
Carpal tunnel syndrome
What is it? This condition occurs when the median nerve that passes through the wrist is compressed, causing pain throughout the hand, wrist and forearm.
How does physiotherapy treat carpal tunnel syndrome? The first priority is to reduce any swelling in the carpal tunnel region and ensure the forearm muscles are functioning properly.
An assessment of the neck and neural system will be done to rule out any problems further up the movement chain.
An assessment of racquet grip and tennis stroke may help to identify any technical issues.
Wrist injuries: famous tennis examples Juan Martin Del Potro has suffered serious injuries to both wrists that have been reported as career-threatening. Nikolay Davydenko is another player to have struggled with a wrist injury.
Patella tendonopathy
What is it? This injury involves pain in the tendon that connects the kneecap (patella) to the top of one of the shin bones (tibia) and is usually caused by overuse. It can be either acute or chronic in nature.
How does physiotherapy treat patella tendonopathy? Management of inflammation and restoration of movement range and control are key factors in this condition early on then a graded loading rehab programme is key.
This condition need not stop a tennis player from playing, but the physiotherapist may suggest modifications to the amount or intensity of play.
Medial collateral ligament (MCL) sprain
What is it?This ligament limits excessive sideways movement of the inner side of the knee joint.
It has close links with the knee meniscus (cartilage) and the anterior cruciate ligament. The Unhappy Triad is the name given when all three structures are injured together.
MCL injuries can vary from overuse strains to full ruptures. A ruptured MCL may be managed conservatively or surgically.
How does physiotherapy treat medial collateral ligament sprain?Immediate treatment involves the PRICE guidelines (above). Protection may be offered in the form of bracing and / or use of crutches. Painkillers can be used but anti-inflammatories should be avoided in the immediate aftermath of the injury.
Restoration of normal range of motion is one of the first targets even if weight bearing is still reduced. Movement control including balance and co-ordination skills will form part of the rehabilitation plan along with hands-on techniques and strengthening.
The physiotherapist will guide the patient through graded exercises from squatting and lunging type exercises to jumping, hopping and landing skills.
Knee injuries: famous tennis examples Rafa Nadal suffers knee tendonitis that requires ongoing management, while Richard Krajceck battled back from a severe knee ligament injury to win further tournaments.
Calf strain
What is it?Injuries to the calf complex can affect the deep and superficial calf muscles, the Achilles Tendon and the Plantar Fascia of the foot.
How does physiotherapy treat calf strain? Immediate treatment involves the PRICE guidelines (above). Protection may be offered in the form of bracing and / or use of crutches. Painkillers can be used but anti-inflammatories should be avoided in the immediate aftermath of the injury.
Restoration of normal range of motion is one of the first targets even if weight bearing is still reduced. Movement control including balance and co-ordination skills will form part of the rehabilitation plan along with hands-on techniques and strengthening.
The physiotherapist will guide the patient through graded exercises from squatting and lunging type exercises to jumping, hopping and landing skills.
Sprained ankle
What is it?The most common injury is a strain to the lateral (outside) ligament but the deltoid ligament on the inside/medial side of the ankle can also be injured. Excessive strain on the ankle where it ‘rolls out’ can cause the lateral ligament to stretch or rupture and medial ligament to compress and get squashed.
How do physiotherapists treat sprained ankle?I mmediate treatment involves the PRICE guidelines (above). Protection may be offered in the form of bracing such as a walking boot, and / or use of crutches. Painkillers can be used but anti-inflammatories should be avoided in the immediate aftermath of the injury.
Restoration of normal range of motion is one of the first targets even if weight bearing is still reduced. Movement control including balance and co-ordination skills will form part of the rehabilitation plan along with hands-on techniques and strengthening.
The physiotherapist will guide the patient through graded exercises from squatting and lunging type exercises to jumping, hopping and landing skills.
If you are suffering with any of these injuries or any others just call for help and support getting you back to your best!
Author
Physioimpulse Chartered Physiotherapists
Archives
June 2024
April 2024
February 2024
January 2024
October 2023
May 2023
February 2023
December 2022
August 2021
July 2021
February 2021
January 2021
July 2020
February 2020
August 2019
July 2019
December 2018
November 2018
October 2018
September 2018
August 2018
July 2018
June 2018
May 2018
April 2018
December 2017
May 2017
February 2017
January 2017
November 2016
June 2016
April 2016
February 2016
January 2016
December 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
February 2015
January 2015
September 2014
August 2014
 RSS Feed
RSS Feed
