 Definition:
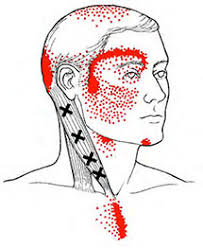
A Myofascial Trigger Point (MTrP) is a discrete, hard, hyper-irritable nodule or ‘knot’ in a taut band of muscle, which is exquisitely tender on palpation. The inclusion of “myofascial” in the name has developed from the view that both muscle and fascia (connective tissue) are likely to be involved in the symptoms. MTrP are often seen as part of Myofascial Pain Syndrome, which is a term used to describe a pain condition that involves the muscle and it’s surrounding fascia. This can be acute or chronic. Active trigger points are associated with spontaneous pain in the immediate surrounding tissue and/or to distant sites in specific referred pain patterns. Strong palpation of the active trigger point can exacerbate a person’s pain complaint and mimics their familiar pain experience. MTrPs can also be classified as latent, in which case the MTrP is physically present but not associated with a spontaneous pain complaint. However, pressure on the latent MTrP elicits local pain at the site of the nodule. Both latent and active MTrPs can be associated with muscle dysfunction, muscle weakness, increased tension and a limited range of motion/reduced flexibility. Background: Muscle pain disorders were first written about in the 1500s. In the 1900s, researchers injected hypertonic saline into various anatomical structures such as fascia, tendon, and muscle in healthy volunteers in order to chart zones of referred pain in local and distant tissue. In the 1950s, Janet Travell and Shannon Rinzler coined the term “myofascial trigger point”, reflecting their finding that the nodules can be present and refer pain to both muscle and overlying fascia. Myofascial Pain and Dysfunction: The Trigger Point Manual is the most comprehensive collection of information on trigger point referral patterns and is used by a wide range of clinicians. However, research is still on-going in this area with the view to further develop our understanding of MPS and the true mechanisms behind MTrP development. Causes: There is general agreement that any kind of muscle overuse or direct trauma/injury to the muscle can lead to the development of MTrPs due to changes in blood flow and the release of chemicals in the body. Muscle overload is thought to be the result of sustained or repetitive low-level muscle contractions, eccentric muscle contractions, and maximal or submaximal concentric muscle contractions, hence causes of MTrP can range from sports training injuries to muscle weakness from lack of exercise; slips/trips/falls/accidents to general muscle strains; and sustained poor postures, including computer use. Generally, myofascial pain resolves in a few weeks with or without treatment. In some cases, however, muscle pain persists long after resolution of the injury; it may even refer to other parts of the body. This heralds the ‘sensitised state’, which is one of the features of a chronic pain disorder, in which the pain itself is the pathology and requires medical intervention for its resolution. I find this fascinating and it is certainly something we see a lot of in clinic, especially given that chronic pain is defined as ‘a pain lasting more than 12 weeks’, which for a lot of people is just a mere drop in the ocean compared to how long they have had their pain. Because of this, MPS has also been associated with other pain conditions such as referred pain from spinal discs and nerves, joint dysfunction like arthritis, tendonitis, migraines, tension headaches, carpal tunnel syndrome, whiplash-associated disorders, pelvic pain and back/neck pain. Interestingly, low mood and sleep disruptions have also been associated with MPS. Treatment: Trigger points may be relieved through non-invasive measures, such as manual therapies, which include post-isometric relaxation, trigger point compression, muscle energy techniques, myofascial release, massage, heat and cold, and stretching. Invasive treatments in our clinics would include dry needling and acupuncture. Invasive medical interventions include injections with local anesthetics, corticosteroids, or botulism toxin. Postural re-training (including pilates), stretching and strengthening exercises, stress management, and mindfulness can also help to address the underlying causes of a person’s MTrPs. This is particularly important in chronic conditions where the chance of recurrence might be more likely due to on-going aggravating factors. Self-myofascial release techniques using a foam roller or spiky ball can be a beneficial part of this self-management. A point regarding referred pain: Referred pain is where a person perceives pain at a location that is different from the site of where the pain originates. Spinal nerves, joints and organs are example of parts of our anatomy that can refer pain. MTrP have specific patterns of pain referral. These charts are easily accessible on the internet and can prove very useful in self-diagnosis. If your pain persists beyond self-help, then it is important to seek professional advice as either not enough is being done to address the underlying aggravating factors that are perpetuating your symptoms, or you may require ‘hands-on specialist treatment’, or it may be that your pain may not be myofascial in origin. If you feel this is something you would like to discuss further, then please get in touch or book in for an assessment with one of our clinicians.
0 Comments
Leave a Reply. |
AuthorPhysioimpulse Chartered Physiotherapists Archives
June 2024
|
 RSS Feed
RSS Feed
ServicesPhysiotherapy Chiropractic Osteopathy Injection Therapy Gait Analysis/Orthotics Shockwave Therapy Bike Fit Running Analysis Sports Massage Pilates |
Get in Touch
|
©
